Character of the Tissues and Organs
The Common Vein copyright 2009
“For every action there is an equal and opposite reaction.” Newton’s third Law
Character, nature, or behaviors are grouped in the same category called “character” for the purpose of simplicity. Character is the most difficult yet usually the most interesting and revealing of all the foundation principles of structure. How is it defined? What is done to establish the character of a structure? Why is an elastic band elastic? Why is rubber rubber? Why is the nature of the liver described as being like jello? How is it established that a person has a nature that is short tempered, impatient calm, cruel, bland or dynamic? How do we establish the character of an abdominal mass and how do we characterize an odd structure like the spleen? How is it established whether a society is cruel or kind? What does it mean if an organism is gram positive, and what does it mean that the rectal examination is Guiac negative?
What is the common theme of these questions and how do we go about answering them under one umbrella principle?
The best way to conceptualize and define “character” is to think of it as a characteristic reproducible response or reaction to an interrogating force (action reaction).
If an elastic band is provoked by pulling the two ends apart and then it is let go, it will react by snapping back to its former length revealing its elastic nature. The interrogating force is a pulling force and the reaction is to return to its former length. Every time the force of pulling is exerted, there is a consistent and predictable reaction. If any structure performs in this manner, then the adjective “elastic” can be assigned as the property or character of the structure.
In the clinical realm one of the ways the character of a structure is assessed is by palpation. The interrogating or provoking action is the application of pressure, a gentle push or gentle pull. A liver may be hard, a mass soft or pulsatile, and skin may lose its elastic tone. Abdominal palpation is often the key to diagnosing pain. An inflamed peritoneal cavity is diagnosed by a slow persistent pressure at the site of the pain, followed by a rapid release of the pressure. If the patient’s reacts with a sudden and severe pain that literally makes him/her jump (sounds a little cruel), then this nature indicates peritonism. Once diagnosed, peritoneal pain takes on a serious and often a surgical direction. If a patient presents with right upper quadrant pain, and cholecystitis is suspected, constant pressure in the right midclavicular line, below the ninth rib, on a deep inspiration may elicit pain as the gallbladder pushes toward and into the examining hand. This is Murphy’s sign, and characterizes the disease as acute cholecystitis.
The color of a structure is also a reflection of its character. By definition, when light falls on an object as an interrogating force it will be reflected absorbed or transmitted. As a result its color will be reflected. Newton observed that light interacts with objects, and some light waves are absorbed, some reflected, refracted, scattered or diffracted. When light falls on (interrogates or reacts with) a red apple, the skin reflects the red waves and absorbs all the other light waves and so the color red is seen. When the eye sees red the tongue anticipates sweetness; green skinned apples (except golden delicious are generally tart. When the light waves interrogate the whites of the eyes of a normal patient, all the colors are reflected, the sclera are considered normal in color. In the jaundiced patient, excess bilirubin causes the yellow or orange spectrum of light to be reflected, and a diagnosis of jaundice is inferred. Thus the color of a structure is a reflection of its nature and is a way we judge its health. If the color is pale or has lost its sheen, then added characterization of the tissue allows us to pass judgment on its state of health or disease.
Tools have been developed to help evaluate the character of structure. The stethoscope, the rubber hammer, and the tuning fork are tools of the early days, carried religiously in the doctor’s bag, and still remain important for bedside examination. The discovery of the microscope and its use in the study of cells and tissues was a significant advance that opened the biological world of the cell and allowed us to evaluate the size, shape, and position as well as the character of tissue.
Imaging
Diagnostic imaging technologies, starting with the discovery of X-rays by Wilhelm Roentgen in 1895, blossomed in the 20th century. Through images we gained insight into the macroscopic structure of the body. Early into the 21st century we are advancing into the structural evaluation of macromolecules and even smaller components. No matter what is discovered, the principles of structure outlined will remain, and characterization will be one of the most challenging.
X-rays are able to penetrate the body, and they react with tissues and organs in a characteristic manner. Similar to the interaction of light with surface objects, X-rays react with deep tissues and are either absorbed, reflected, or transmitted. Air in the body allows the X-rays to go right through and the result is for air to appear black on the X-ray screen. Soft tissue allows some X-rays through and reflects others, so the tissues have a gray color on the film. Bone or barium mostly blocks the X-rays and so the structures appear white. Not only does this technique allow inner structures to be identified, it also allows analysis of their parts, size, shape, and position. Most importantly, X-ray technology marked the beginning of non invasive characterization of tissue.
CT scanning technology advances the technique by adding interrogative X-rays from multiple angles around the body. This technique, combined with an ever evolving computer technology, has taken the non invasive evaluation of macroscopic structure to greater heights. The result has been a significantly widened grayscale, an ability to assign units of density, called Hounsfield units, and an ability to reformat structures in any desired plane. The latter enabled the first practical objective means of characterizing tissues in clinical radiology. If a 5cm renal tumor has a 3mm component with a density of -30Hounsfield units, the presence of a small amount of fat in the tumor is confirmed. A benign tumor called an angiomyolipoma is diagnosed. In this circumstance the tumor is left alone, and surgery is avoided Prior to the era of CT technology this mass would have required surgical removal of the whole kidney.
Ultrasound technology interrogates body structures with high frequency sound waves which are reflected, absorbed or transmitted. This action and interaction enables characterization of tissue in much the same way described by the interaction of light waves on the surface structures, and X-rays on the deep structures. MRI technology is slightly different since it uses a strong magnetic field to align the protons of the body, (60-70% of body content), and then adds a brief radiofrequency pulse that changes the alignment of the protons (usually 90 degrees). The protons are then allowed to relax back to their baseline position within the magnetic field. The time it takes the protons to relax, is defined as the character of the tissue being imaged. Thus the protons within the matrix of the liver will have a normal and predictable pattern, and the spleen will have its characteristic but different pattern. If a malignant squatter invades the liver or the spleen, its pattern or character will be different. It is this difference that allows recognition.
There are many different MRI sequences which are each designed to emphasize tissue features or characteristics. For example, T2 weighted images are sensitive to the presence of water. A cyst in the liver or kidney, normal cerebrospinal fluid and the fluid filled gallbladder will all be bright on T2 imaging. Diffusion weighted sequences are sensitive to Brownian motion of extracellular water, or the lack of it. These are extremely helpful in the diagnosis of acute infarction of the brain. The technology can reflect the presence of acute hemorrhage, and can date the bleed by differentiating between deoxyhemoglobin in intact red cells, (0-2days), the change to methemoglobin, (2-14days), and then the change to hemosiderin laden macrophages in the chronic stage (14days to months). The most useful and most unique advances provided by MRI technology have been its non invasive ability to characterize tissue.
Pathology
In order for the histologist or pathologist to characterize tissue and cells, he/she employs chemical stains. These represent a chemical interrogation of the cells. The hematoxylin and eosin stain (aka H&E) is one of the most widely used stains in histology and histopathology departments. It involves applying a basic stain called hematoxylin that will color basophilic structures like the nucleus, blue. The cytoplasm stains pink, as do extracellular and intracellular proteins. In cancer, the blue nucleus is even bluer of the aberrancy of the nucleic acids. This characteristic is called hyperchromatic by pathologists, and is one of the characteristic features of cancer. Little crabs are not seen. Instead the essence of the disease is in the chromatin. This is where the beginning of understanding the disease and potential treatments are being targeted. Non pathologists who have no clue to what they are seeing under the microscope, when seeing too much blue refer to an inside joke of “blueness is badness”. This of course is in reference to the hyperchromicity of cancer.
Chromosome banding is the technique used to characterize chromosomes. Quinacrine, a fluorescent dye is used in a technique called Q banding. After digesting chromosomes with trypsin, Giemsa stain is used in the G banding technique, and the stain is also used after the chromosomes are treated with acid and base and it binds to the centromeres of the cell. This is called C banding (centromeric heterochromatin banding). Each chromosome has a unique normal banding pattern that can be viewed and evaluated just like the bar code on a box of Wheaties.
Nanorobotics is a fascinating hypothetical extension of nanotechnology that utilizes both nanotechnology and robotics to interrogate and evaluate the body and its tissues. Its intended purpose is identification of specific tissues (histonavigation ) by characterization using the speed of sound through the tissues, spectral transmission of optical wavelengths, cell membrane electrical conductivity, characteristic chemical signatures, and surface antigens (Freitas).
The fields of MRI, immunostaining and nanotechnology are cutting edge and wide open for advances, but the principles of characterization remain true, whether via simple palpation or with a nanorobot racing around on a red cell interrogating the tissues. Characterization captures a reproducible response or reaction to an interrogating force.
Principles
Air
 Air Air |
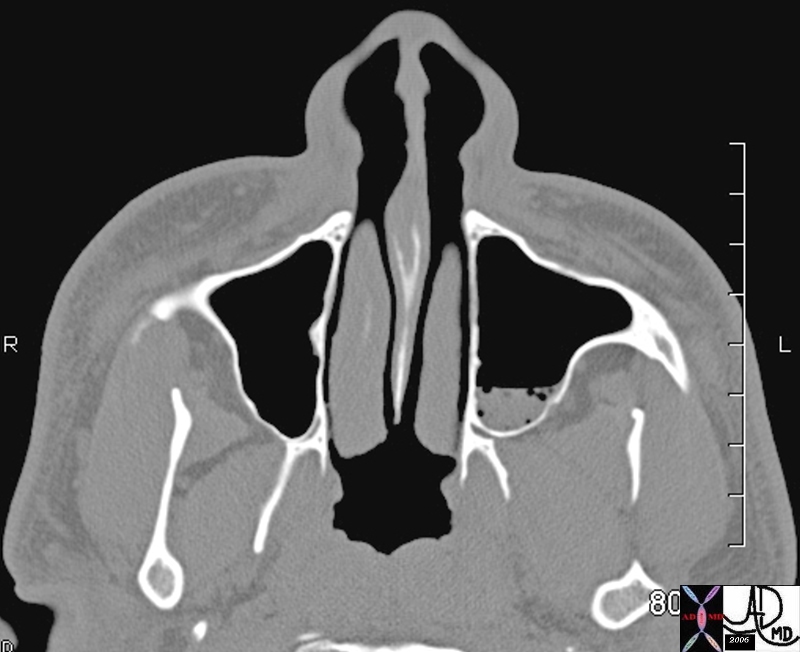
| 46308 skull maxillary sinus fx air fluid level fx air bubbles fx complex fluid dx acute sinusitis CTscan maxillofacial Davidoff MD |
Air in Gallbladder Fossa |
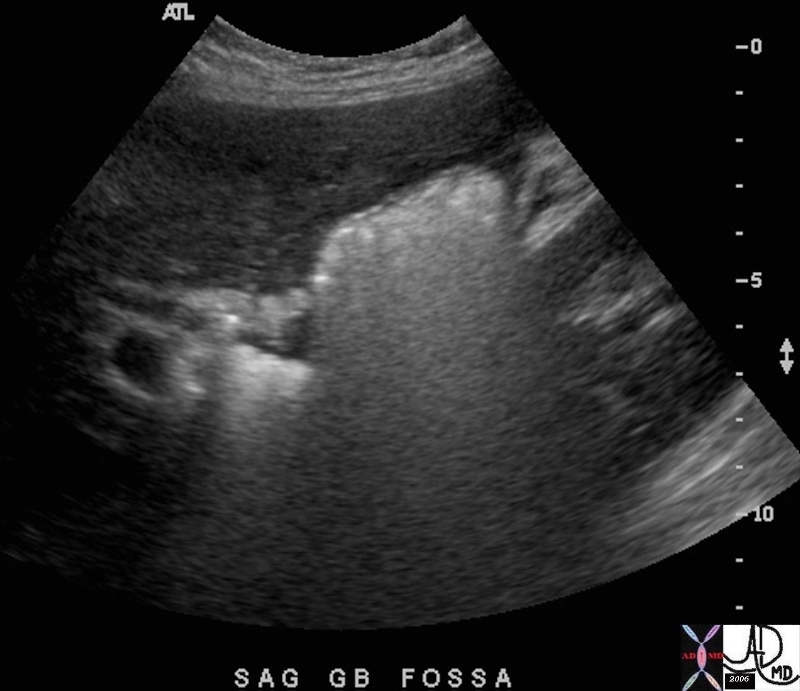
| 46625 gallbladder fossa s/p cholecystectomy with gelfoam packing of fossa fx echgenic collection in gallbladder fossa dx air within gelfoam USscan Davidoff MD |
Methane or Nitrogen in a Cholesterol Stone |
| 70269c02 gallbladder air methane nitrogen gas cholesterol stone isodense with bile fat subtle change CTscan |

Tissue Necrosis |
| 86400.8s The RFA probe in this instance is in a liver metatastasis in a patient with an unknown primary. The bubbles sen in the lesio represent necrosis following ablation. It is not common to see immediate macroscopic results. This lesion is about 7cms in diameter. code liver hepatic metastasis unknown primary 7cms necrosis tumor air bubbles radiofrequency ablation copyright 2009 Courtesy Ashley Davidoff MD all rights reserved |
Calcium
Calciun in the Mitral Valve and Pleura |
| This chest CT through the middle of the left ventricle (LV) shows some calcification athe base of the mitral valve (MV) focal calcification of the anterior leaflet and and increase density of both leaflets. This patient had no known mitral valve disease and the findings most likely represent dystrophic calcification due to mucinous degeneration. Courtesy Ashley Davidoff MD. 19729 code heart mitral valve MV calcification cardiac imaging radiology CTscan |
Calcified Myocarditis |
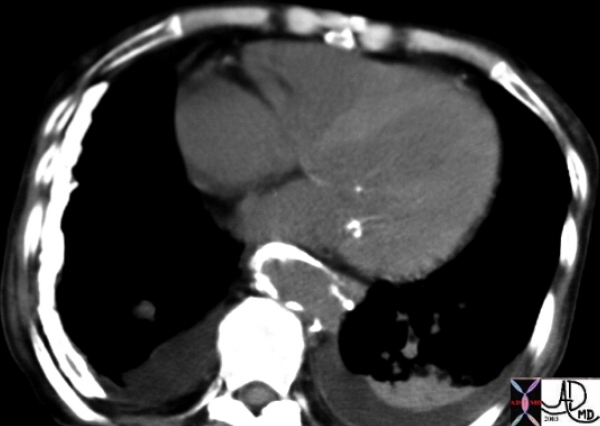
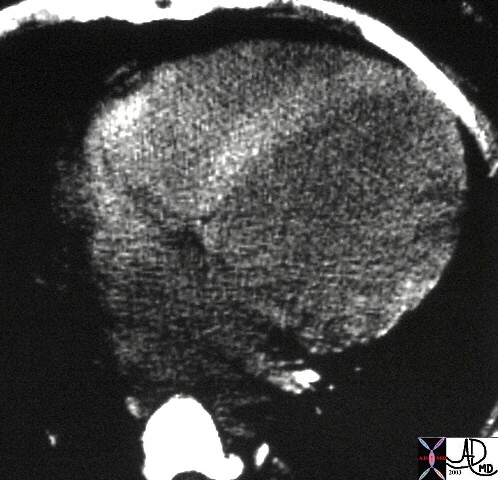
| This is a CT of the chest at the level of the heart filmed on narrow windows showing a dense ventricular septum. The autopsy specimen showed calcific myocarditis. Courtesy Ashley Davidoff MD 24672 |
Eggshell Calcification |
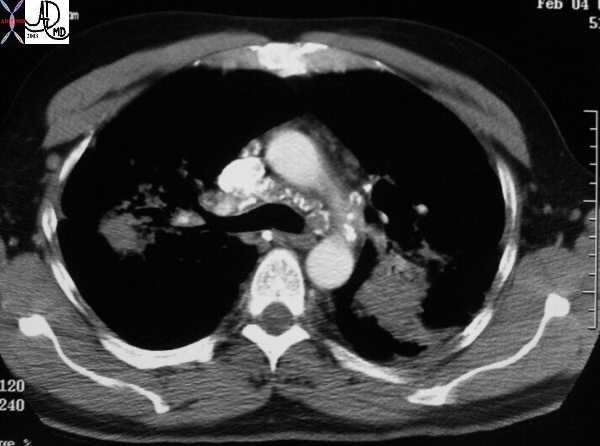
| This CT shows classical long standing confluent fibrosis in the upper lobes in this patient with sarcoidosis. The egg-shell calcification of the mediastinal nodes is also classical as is the upper lobe predominance with apical and posterior segmental predominance. Courtesy Ashley Davidoff MD 29128 |
Popcorn Shape |
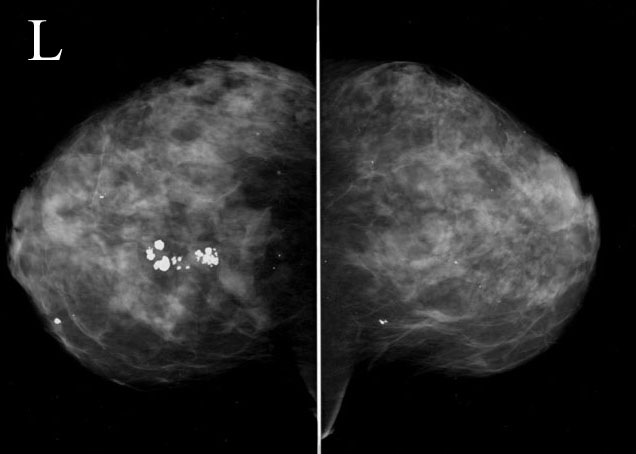
| This mammogram shows large popcorn shaped calcifications in the left breast characteristic of an involuting fibroadenoma. 42748 Courtesy Priscilla Slanetz MD MPH |
Pleural Calcification – Asbestos |
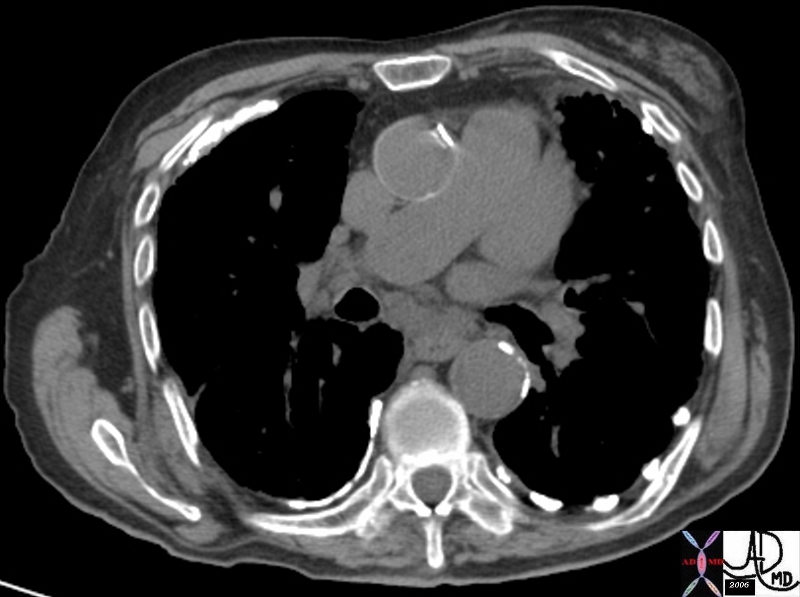
| 46624 hx 77 year old male with SOB breast pleura fx gynecomastia pleural calcification dx asbestos related disease dx asbestosis CTscan Davidoff MD 46621 46623 46624 46622 |
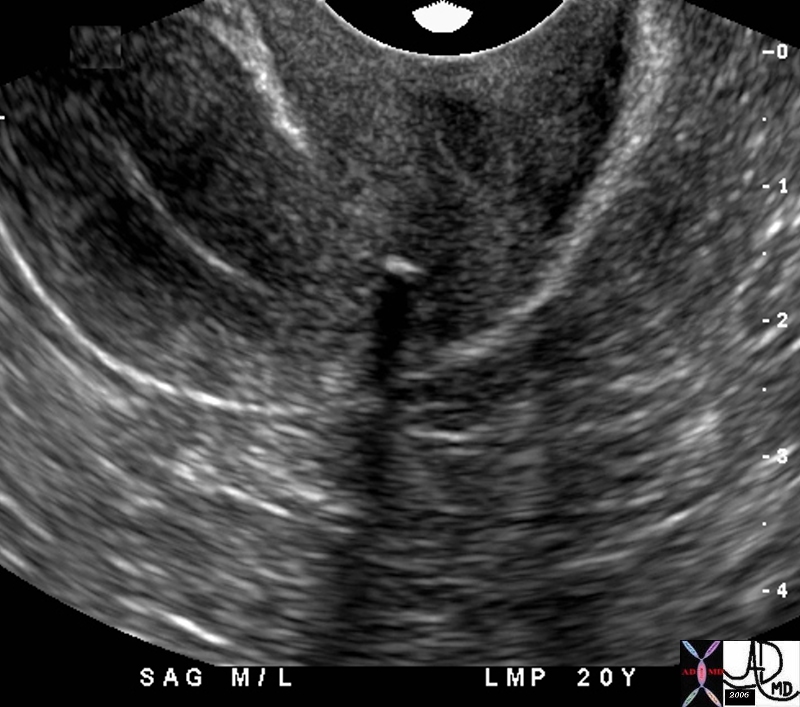
Shadowing of Calcium on US |
| 46327 LMP 20 years ago uterus endometrium calcification shadowing lower uterine segment dystrophic calcification dx degerated fibroid imaging USscan Davidoff MD |
When Calcium Means Bad Things
Porcelain Gallbladder |
| 47683c01 gallbladder fx calcification in wall calcified wall dx porcelain gallbladder CTscan Davidoff MD |
Water
Water density
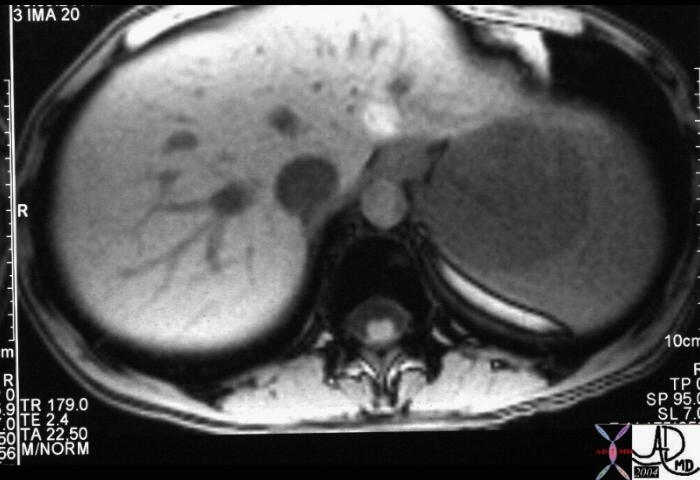

| Splenic Cyst |
| 22933 22934 spleen + fx mass + fx T2 bright + dx splenic cyst imaging radiology MRI scan + T2 neoplasm benign cyst tumor fluid |
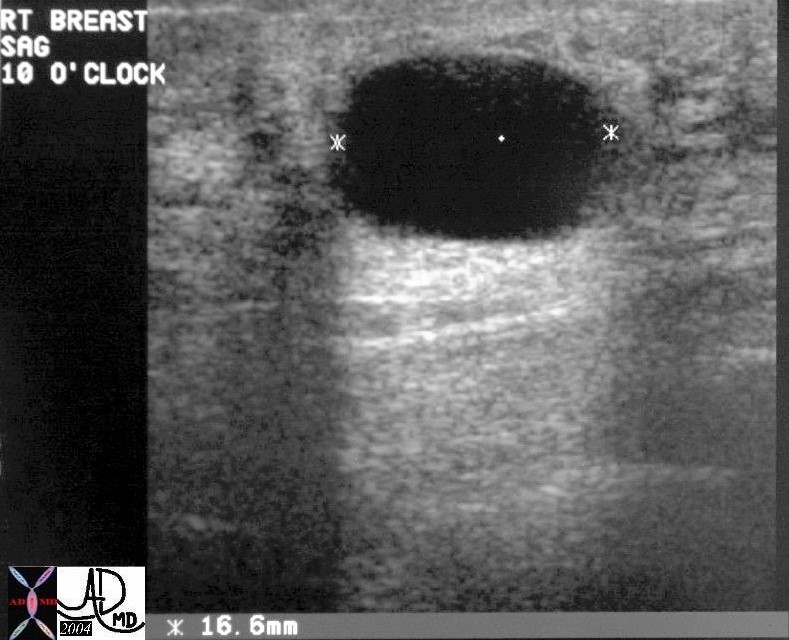
| Cyst |
|
A cyst is noted on this ultrasound in the breast of a young woman with a palpable mass. This entity is part of the fibrocystic entity discussed above and most commonly presents as a disturbing mass. Ultrasound is the study of choice when this condition is clinically suspected. Note that the cyst has no internal echoes, the wall has no evidence of neither focal nor diffuse thickening and there is superb through transmission of sound. Courtesy Priscilla Slanetz MD MPH 28241 |

Through Transmission |
| 49463 cervix fx cysts anechoic through transmission backwall enhancement dx Nabothian cysts USscan Davidoff MD |
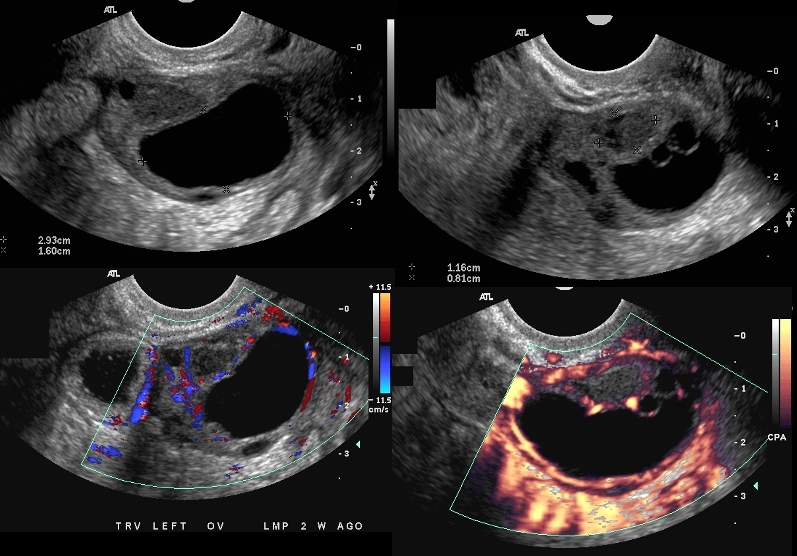
| Complex Cyst |
| 46557c01 ovary fx cystic mass with thickened loculations fx enhancing wall dx neoplasm neoplastic change dx complex cyst needs follow up USscan doppler Davidoff MD |
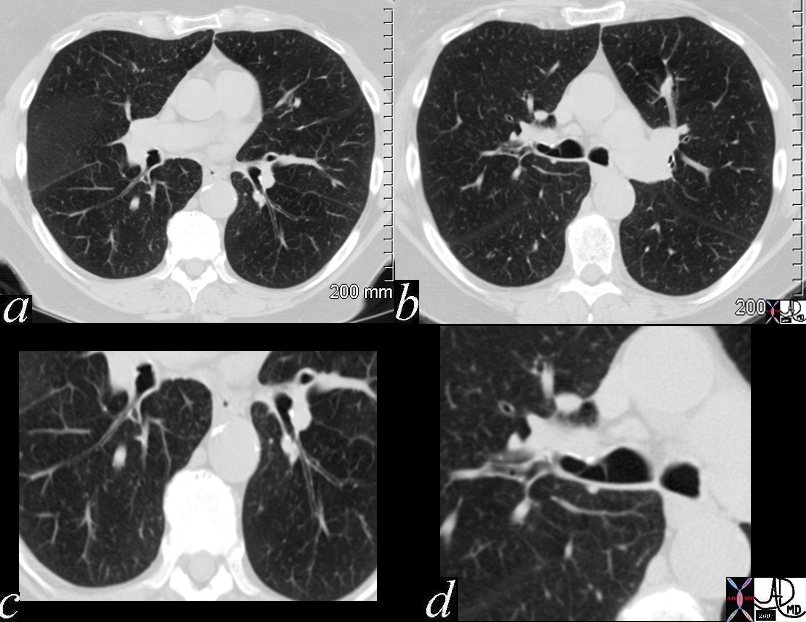
Strand of Mucus – Chronic Bronchitis |
| 70217c01 lung bronchus bronchi left mainstem bronchus lower lobe bronchi thickened walls strand of mucus dx chronic bronchitis character mucus CTscan Davidoff MD |
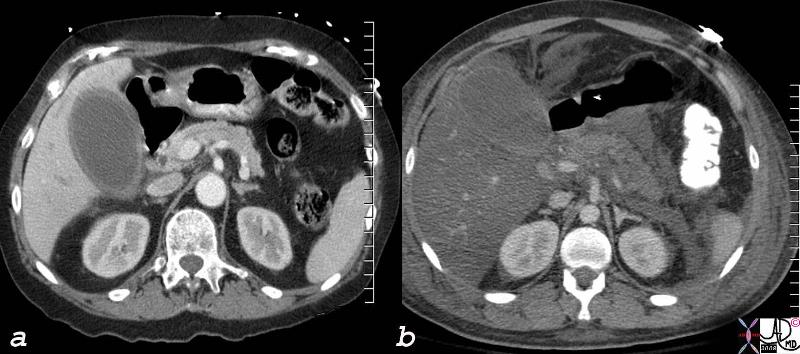
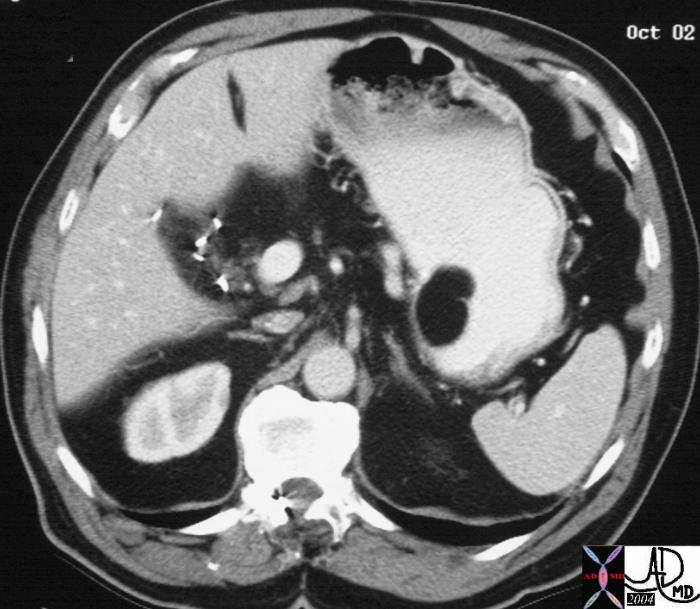
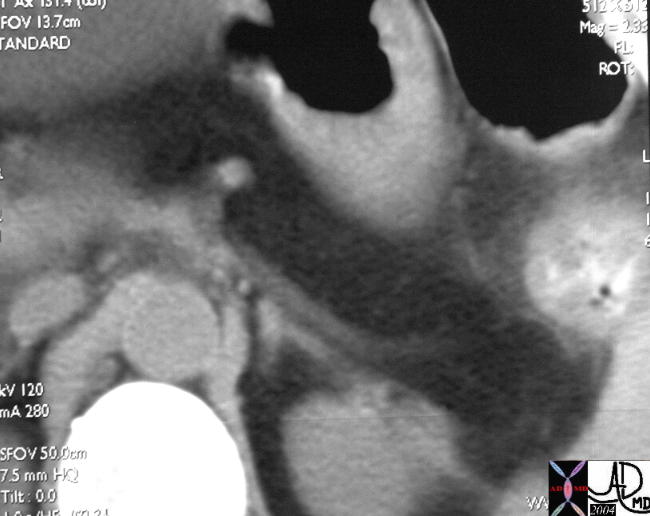
Relative Density – in Acalculous Cholecytitis and in Fatty Liver |
| 78606c.8s liver normal liver abnormal fatty change 777017 = a = acalculous cholecystitis b= pancreatitis with steatosis hepatization of the gallbladder density of the liver is the same as the bile in the gallbladder CTscan Courtesy Ashley Davidoff MD copyright 2008 |
Fat
Fat density
Normal Breast Tissue |
| 48066 breasts fat no glandular tissue character size shape normal variant CTscan Davidoff MD |
Lipoma of the Stomach |
| 19935 stomach gastric + mass fat lipoma + imaging radiology CTscan |
Fatty Pancreas |
| 22995 pancreas + fx fat + pancreas + fx fat + fatty atrophy + dx cystic fibrosis + imaging radiology CTscan C- + dx cystic fibrosis + imaging radiology CTscan C- |
|
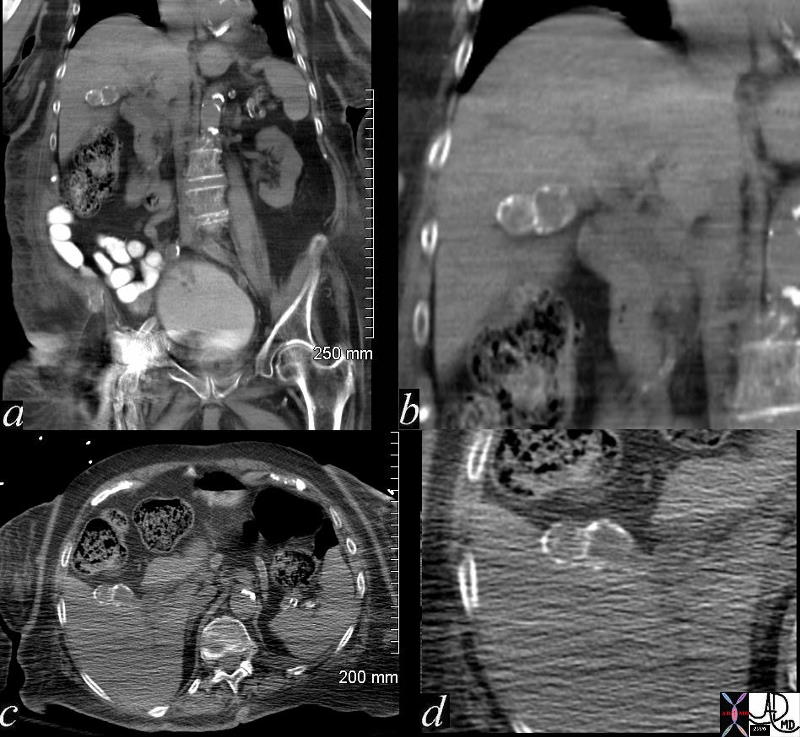
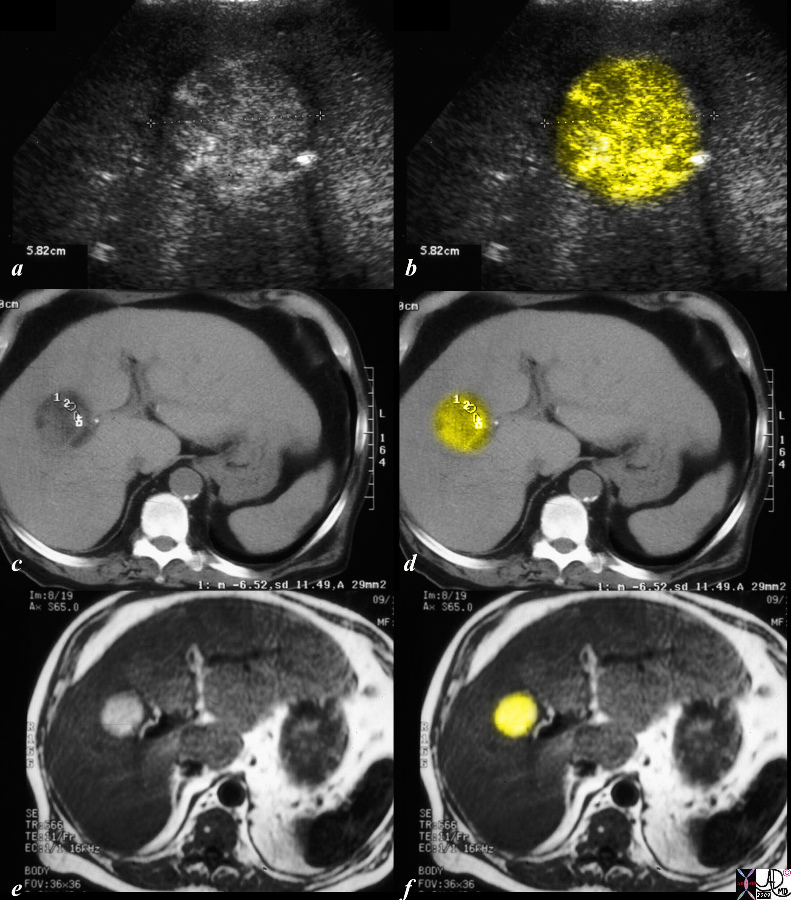
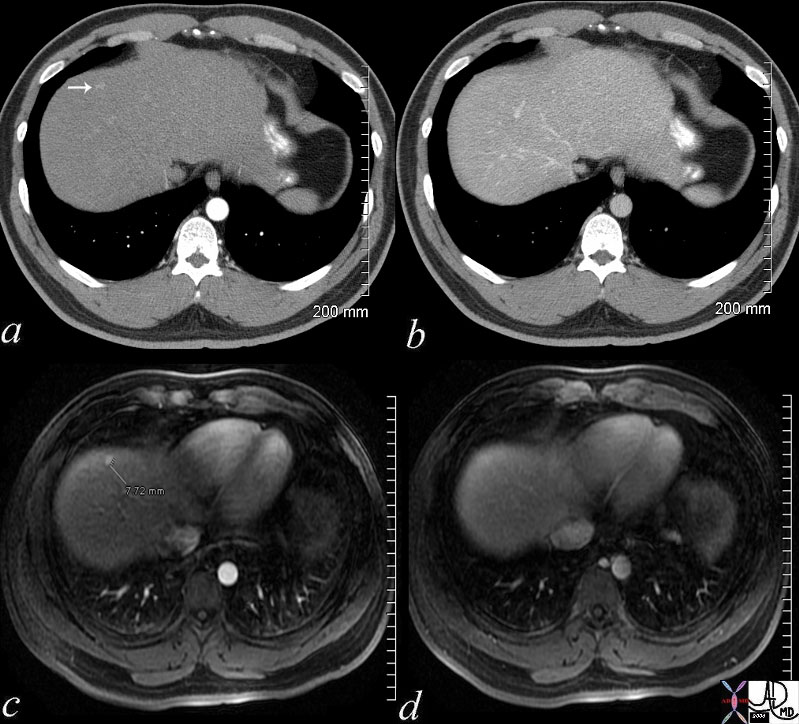
Fat in HCC |
|
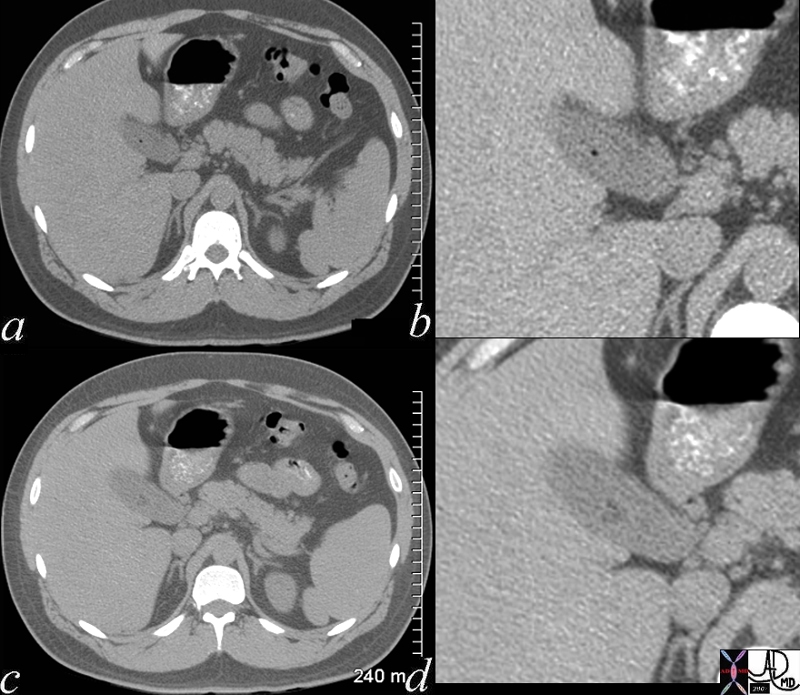
The series of US (a,b) CTscan (c,d) and T1 weighted MRI all reveal the same finding – a fat containing lesion, characteristic and pathognomonic for practical purposes of an HCC. The ultrasound shows an echogenic mass, the CT shows a a density o -6Hu and the MRO shows T1 bright lesion. All these features are characteristic of fat within the lesion. Not also the prominent artery seen at 3 o’clock on all sequences. Surgical removal of this almost 3cms lesion proved to be an HCC. code liver hepatic cancer HCC hepatocellular carcinoma hepatoma CTscan USscan ultrasound MRI T1 weighted Courtesy Ashley Davidoff copyright 2009 all rights reserved 86367c02.9s |
Soft Tissue
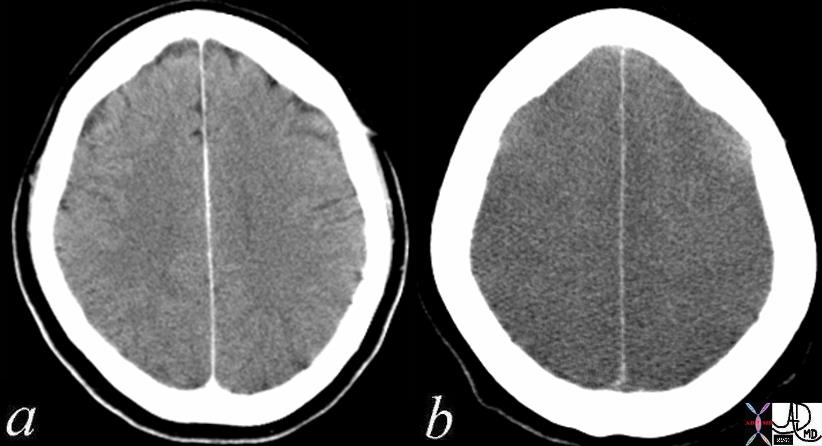
Normal – 4 months Prior and Folllowing Cardiopulmonary Arrest Loss of Gray White Differentiation |
| 70134c01 hx 52 F post cardiac arrest brain cerebrum gray matter white matter gray white differentiation gray white distinction sulci gyri loss of gray white differentiation hypodense dx anoxic injury with diffuse global cerebral edema Davidoff MD Loss of consciousness occurs within 10-15 seconds of cardio-pulmonary arrest. Irreversible brain damage can occur within 5 minutes. gray matter of the brain, particularly the frontal lobes have highest metabolic needsThe occipital, parietal, and temporal lobes and basal ganglia and cerebellum are lower. brainstem lowest needs |
Soft tissue density
Blood
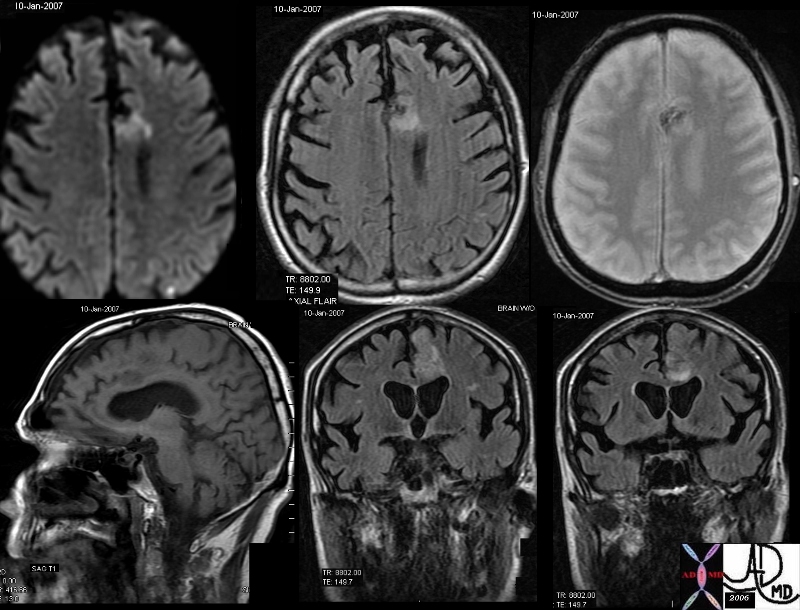
Acute Blood |
| 46098c01.800 brain frontal lobe fx hyperintense focus diffusion images fx hyperintense T2 weighted STIR fx dark GRE fx dark T1 dx hemorrhagic infarction hemorrhage acute bleed dx acute hemorrhagic emboli MRI Courtesy Ashley Davidoff |
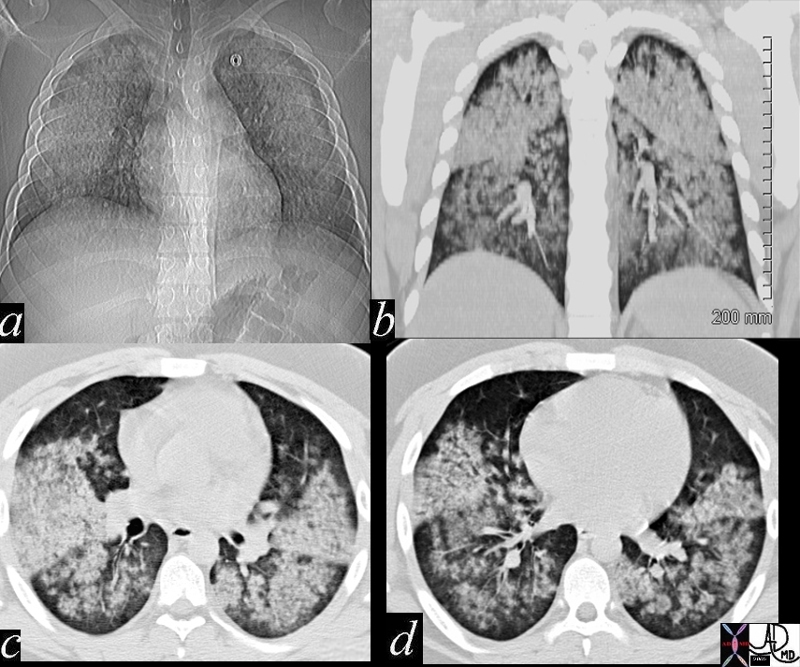
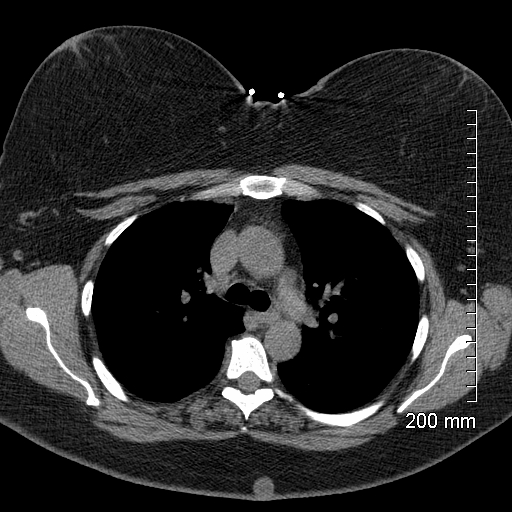
Wegener’s Granulomatois Acute Hemorrhage |
|
47711c01 20 year old male presents with hemoptysis and renal failure chest lungs upper lobes lower lobes infiltrates acinar infiltrates fluffy infiltrates almost symmetrical fx bilateral pulmonary infiltrates renal biopsy dx Wegener’s granulomatosis with pulmonary hemorrhage blood character CTscan Daviddoff MD 47711c02
|
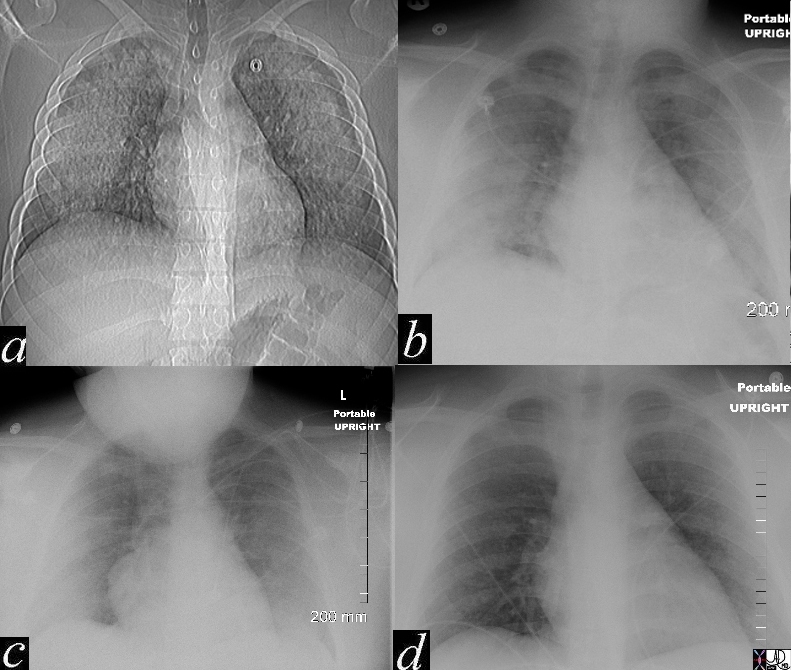
Wegener’s Granulomatois Acute Hemorrhage Rapid Clearing
|
| 47711c02 20 year old male presents with hemoptysis and renal failure chest lungs upper lobes lower lobes infiltrates acinar infiltrates fluffy infiltrates almost symmetrical fx bilateral pulmonary infiltrates renal biopsy dx Wegener’s granulomatosis with pulmonary hemorrhage blood character CTscan Daviddoff MD 47711c01 |
Elastic Nature
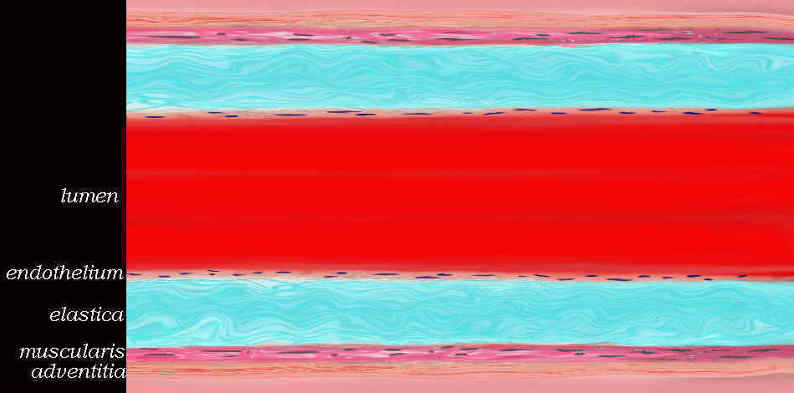
Elastic Artery |
| 47678b04.800 artery aorta histology character normal endothelium media adventitia tunica elastica tunica muscularis |

Systole and Diastole in the Elastic Aorta |
| This image of the theoretical functioning of the role of resistance and outflow enabling the infrarenal aorta to function as second pump. In systole (b) the suprarenal artery is expanded by the pulse but is relatively decompressed by the the low resistance and high flow renal arteries. The infrarenal aorta is relatively more expanded in systole (b) since the iliac arteries offer a relative resistance. This increased resistance causes the elastic tissue in the aorta to stretch (b) so that the recoil in diastole (c) results in a sustained forward moving force assisting the blood to get to their most distal destination – the feet. Courtesy Ashley Davidoff MD. 24877c |
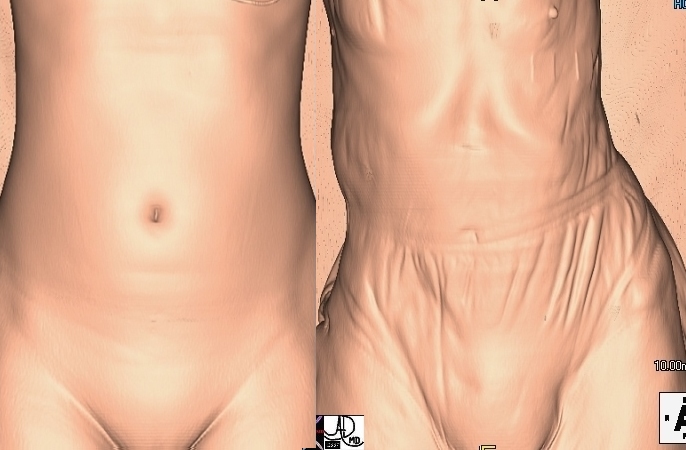
Loss of Elasticity |
| 49609c03 abdomen health disease young old time cycle elastic elasticity order disorder Davidoff MD 49609c02 |
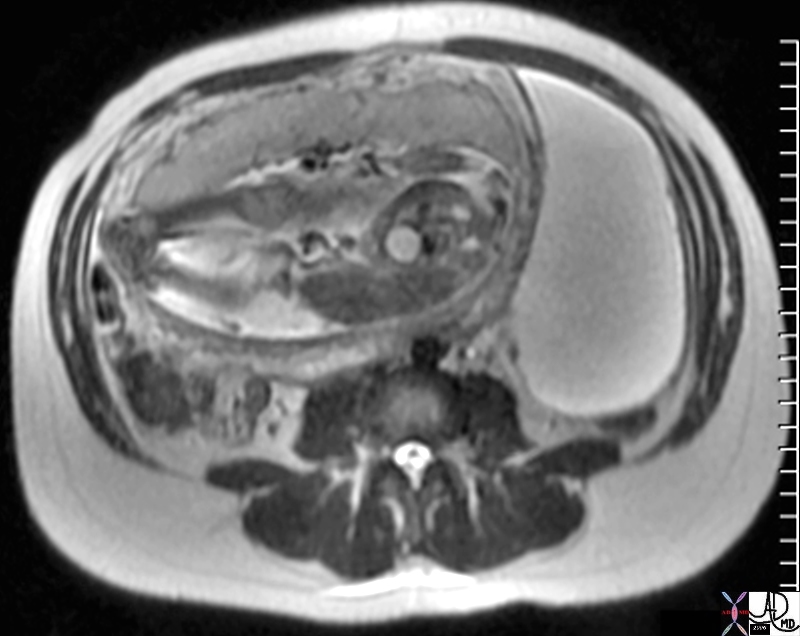
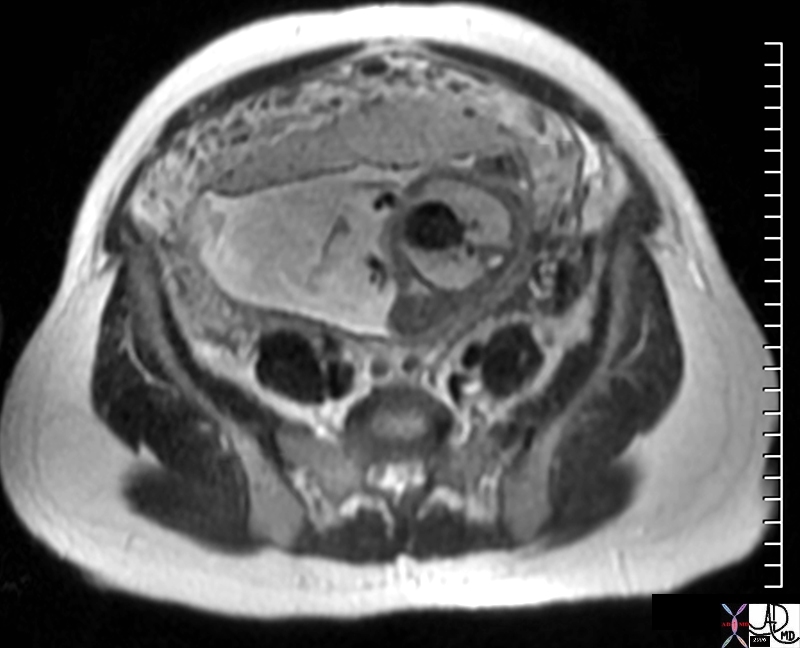
Yielding to Pressure |
| 47753 24 week pregnancy ovary OB fetus amniotic sac placenta bladder fx large left ovarian cyst compressed by pregnancy pressure character water T2 bright MRI scan Davidoff MD concepts |
Mobility
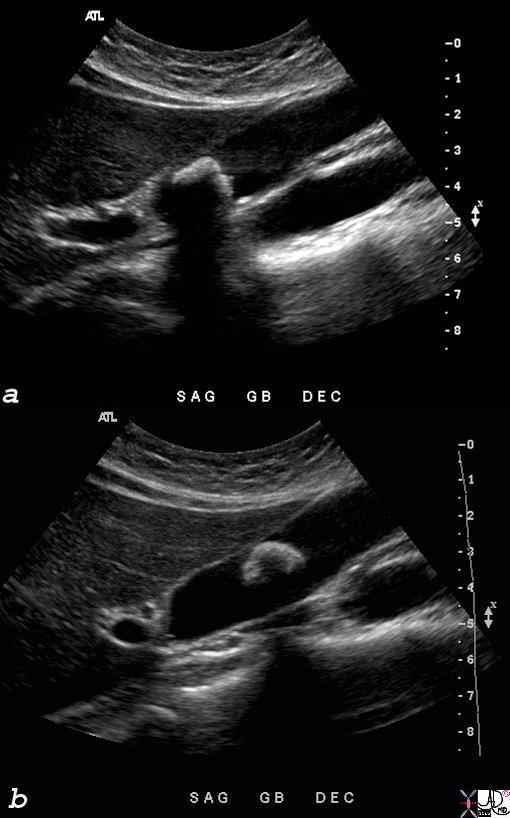
Mobile Stone |
| 46462c01s gallbladder moderaste size shadowing mobile stones cholelithiasis USscan ultrasound Courtesy Ashley Davidoff MD copyright 2008 |
Character and Time
Contrast Enhancement Patterns
Contrast
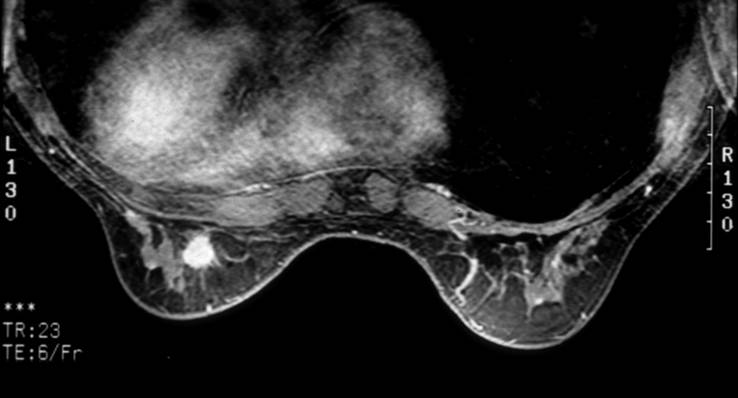
Enhancing Spiculated Malignant Mass |
| The finding on this contrast enhanced MRI is a mass in the left breast that is hypervascular and has a spiculated border. The pathology on this case was an invasive intraductal carcinoma. Courtesy Priscilla Slanetz MD MPH 42982 |
 Small arterial fed liver lesion Small arterial fed liver lesion |
| 48369c03 40 male with hepatitis B liver fx hypervascular lesion seen in early arterial phase only with rapid wasout dx HCC hepatoma hepatocellular carcinoma capillary hemangioma characterisation characterization blood flow CTscan MRI Courtesy Ashley DAvidoff MD |

Liver Lesion s/p RFA |
| 46573 liver fx mass with avascular central region and enhancing rim space occupying disease dx liver metastases metastases dx adrenal mestastasis dx primary lung carcinoma post radiofrequency ablation RFA of large liver lesion CTscan Davidoff MD |
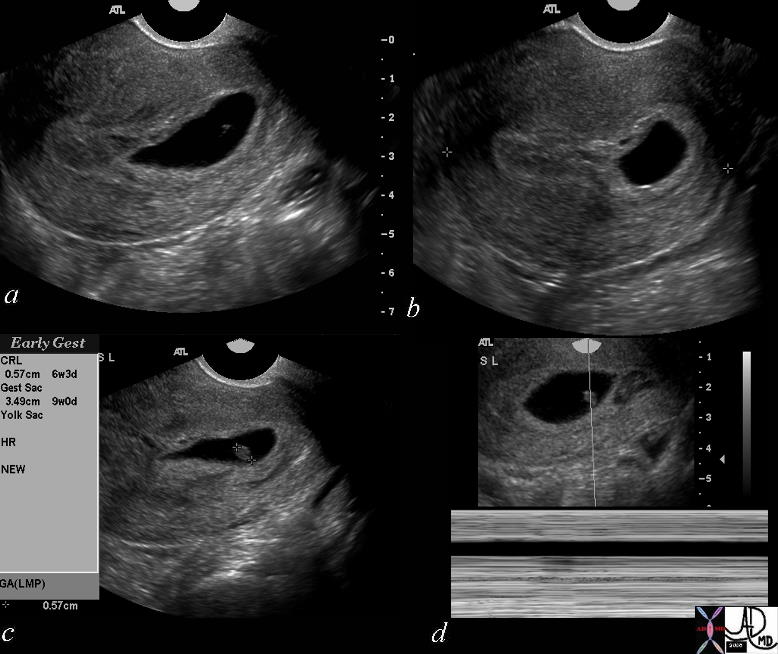
Lack of Doppler Flow – Death |
| 46592c01 uterus OB pregnancy fetal demise spontaneous abortion shape size position heart rate USscan Davidoff MD death |
Benign Characteristics
Benign Disease
| Fig. 1
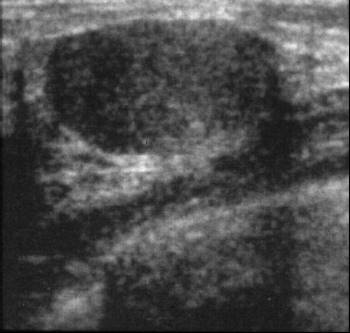
Fig. 2 Smooth Margins Well Circumscribed Benign Mass |
| A mammogram on the left shows an ovoid mass which is hypoechoic with smooth margins. These findings are characteristic of a benign lesion and could represent a cyst or fibroadenoma as the most likely causes. The US on the right shows a well circumscribed solid mass characteristic of an adenoma. Courtesy Priscilla Slanetz MD MPH 42913 42914 |

|
Popcorn Shape |
| This mammogram shows large popcorn shaped calcifications in the left breast characteristic of an involuting fibroadenoma. 42748 Courtesy Priscilla Slanetz MD MPH |
Malignant Characteristics
Malignant Characteristics
Shape
Stellate |
| 69595b05.800 star stellate corona radiata spiculated aggressive cancer carcinoma Davidoff art |
Davidoff photography
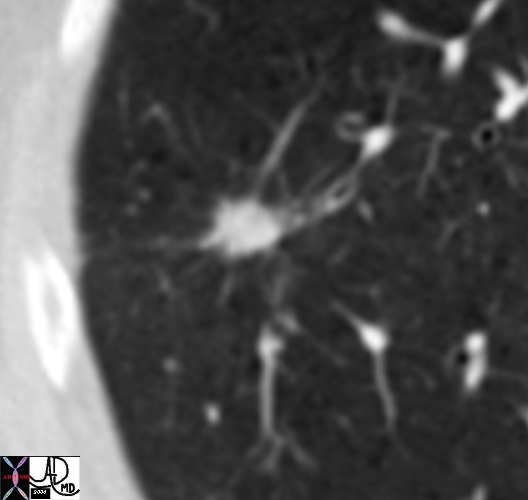
Spiculated Lung Nodule |
| 46361b01 lung fx spiculated nodule dx carcinoma CTscan Courtesy Ashley Davidoff MD |
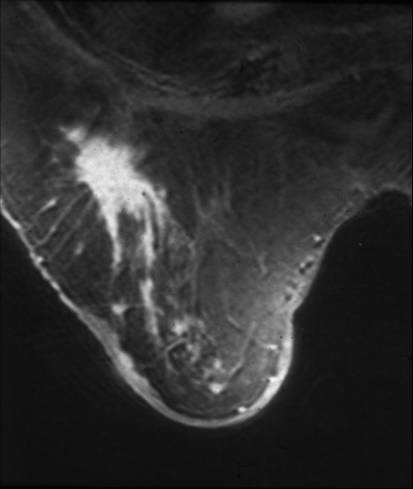
Spiculated Mass in the Right Breast |
| This is an MRI of the right breast of a 78 year old patient with a remote history of invasive lobular carcinoma. The finding on the MRI is characterized by an enhancing spiculated mass. Recurrent carcinoma was present at pathology. Courtesy Priscilla Slanetz MD MPH 42977 |
Aggressive Growth
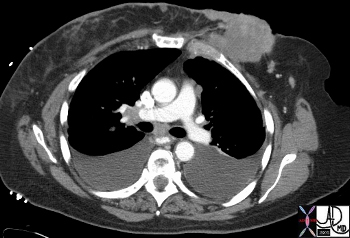
Aggressive Mass Invading the Chest Wall |
| The CT reveals an obviously aggressive lesion in the left breast of a 66year old female. It is extending as an irregular mass invading the chest wall posteriorly and projecting through the skin anteriorly. Courtesy Ashley Davidoff MD 43615 |
Complexity
Relationship to Gravity
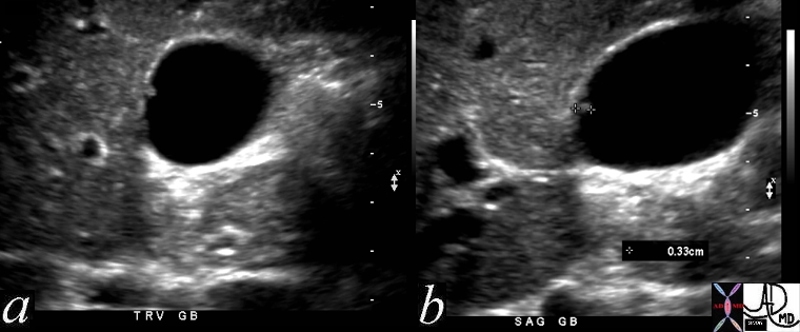
Gallbladder Polyp surrounded by fluid – 3mms |
| 47017c01 gallbladder fx nodule fx adeherent fx non dependant size character through transmission dx gallbladder polyp Davidoff MD |
Hard and Soft
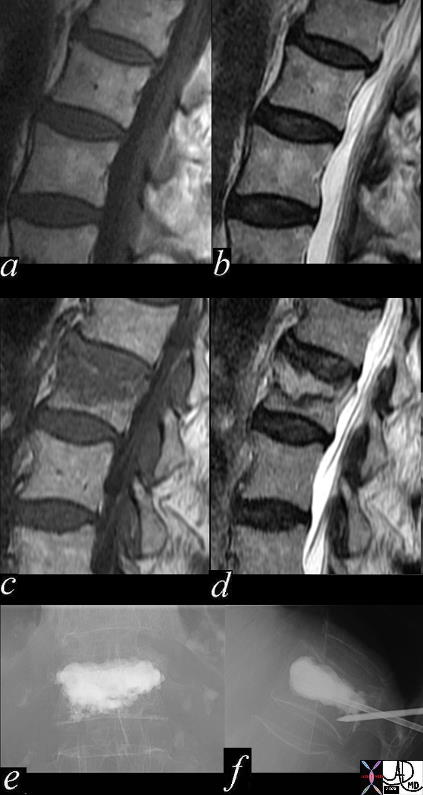
Compression and Treatment – Soft to HArd |
| 47187c02.800 back spine lumbar spine L5 compression fracture vertebraplasty MRI Davidoff MD Dr Ram Chavalli |
Elastic
|
Young and Aging Normal Elasticity and Aging Elasticity |
| 49609c03 abdomen health disease young old time cycle elastic elasticity order disorder Davidoff MD 49609c02 |
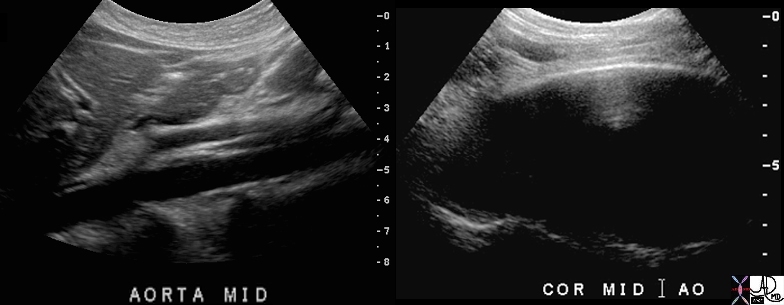
Normal aorta and Abdominal Aneurysm – Pressure Tension and Laplace’s Law |
| 70027c01 aorta abdomen abdominal aortic aneurysm normal aorta TCV applied biology AAA USscan Davidoff MD |

Pressure Tension Radius Laplace’s Law |
| This image shows a famous cardiologist, Dr Jonathan Fisher performing as Zippy the clown revealing and exaggerating the difficulty with surface tension and radius in the early stages of blowing up a balloon. Courtesy Ashley Davidoff MD. 60730b01 code lung physiology balloon surface tension surfactant alveolus alveoli radius principles |
Infarction
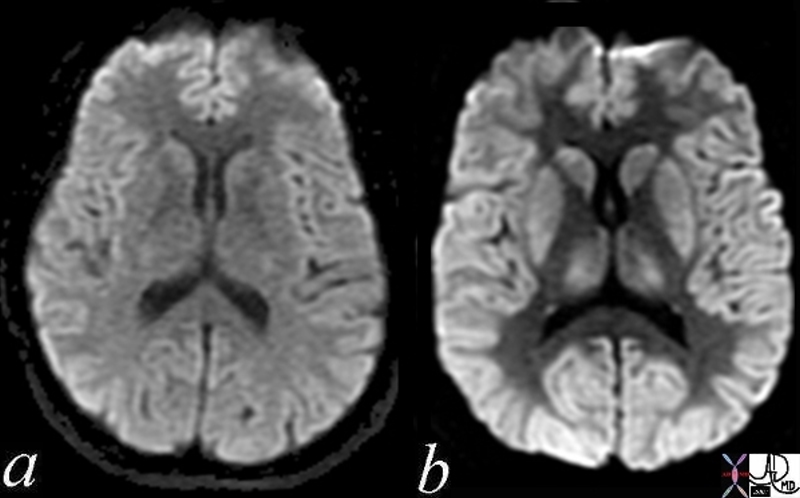
Normal and Global Ischemia after Cardiac Arrest |
| The two images represent a diffusion weighted MRI image which measures Brownian motion of molecules. In acute infarction there is restricted Bronian motion of the affected area and the image can be manipulated to present this a s a bright region. In this case the acute infarction or ischemia (b) is relatively bright compared to the white namatter and compared to the gray matterof the normal (a)
49433c02.800 brain cerebral cerebrum white matter gray matter basal ganglia fx increase intensity in gray matter relative decrease in intensity in white matter dx global ischemia question brain death probable irreversible brain death cerebral infarction s/p arrest MRI DWI diffusion weighted imaging normal and abnormal Courtesy Ashley Davidoff MD |

Weak to Strong – Soft to Hard |
| 49586c01 bone thoracic spine compression fracture trauma cement reenforcement wek link units to unity units to dysunity joints treatment CTscan Davidoff MD |
Character Change With Treatment

Chemotherapy – Before and 6 weeks After – Metastatic Small Cell Lung Carcinoma |
| 70248c01 liver metastattic small lung carcinoma with diffuse metatstattic disease to the liver )hepatic metastases metastasis before and after treatment 6weeks post chemotherapy successful result size change character change CTscan Davidoff MD 5star |